|
William Brightman DC, MS, MEd When I hear a patient say that their shoulder is in pain the first thing I ask them to do is point to where the pain is coming from. The patient may point to an area in the vicinity of the shoulder like the base of the neck (cervico-thoracic region), the collar bone and upper chest (clavicular-pectoral region), or the shoulder joint (glenohumeral) itself. They may also point to their shoulder blade close to the mid back (scapulo-thoracic region) to identify their source of pain. In other words, the term “shoulder” can cover a large region for most patients trying to describe their pain. Fortunately, most musculoskeletal pain can be identified with a complete hands on physical exam. Once the tissue(s) are identified and tested then a conservative approach can commence. The patient should start noticing improvement within the first few treatments. The following is a short incomplete list of problems that might be discovered in the exam. Rotator cuff dysfunction including strain, tendonitis (inflammation), tendinosis (adhesions), impingement (pain when lifting arm away from or behind body), bursitis (inflamed bursa sacs that are irritated from friction), and adhesive capsulitis (frozen shoulder). Other musculoskeletal problems of the shoulder might require more advanced diagnostic testing such as x-rays, MRI’s and CT scans and may capture tears, arthritis (several kinds), avascular necrosis, fractures, infections, and tumors.  Rotator cuff muscles of the shoulder (they are the core muscles in the shoulder and responsible for stabilizing and moving the joint is several planes of motion). There are non musculoskeletal problems that may contribute to shoulder pain as well and should be ruled out prior to treatment. Conditions such as gallbladder disease which classically refers to the right scapulothoracic region and of course heart attacks have been known to refer pain to the left shoulder as well the mid back region. Lung conditions such as a blood clot (pulmonary embolism), infection, and tumors may also refer to the shoulder region. Other internal organs may refer pain to the shoulder including pancreatitis, an ovarian cyst, and an ectopic pregnancy to name a few. Thankfully, non musculoskeletal shoulder pain is the exception and not the rule. In my office, I collaborate with other specialists if we are suspicious of chronic shoulder pain that does not respond to conservative care and may be from non-musculoskeletal sources. Fortunately, most shoulder problems are mechanical in nature and are the result of either muscle tightness, adhesions, and joint restrictions in the neck and upper back. Repetitive stress from poor posture and ergonomics will contribute to shoulder pain slowly and insidiously over time. This is why many patients will say that it just came “out of nowhere” usually upon awakening from a night's sleep. It is not the fact that they “slept wrong” but rather the poor mechanics they use while they sit, stand, and sleep over a period of time. This will ultimately cause an imbalance in the neck, upper back and shoulder region. It is often accompanied by a shoulder impingement. Shoulder impingement is a reduction in the gap between the ball and socket where one of the rotator cuff muscles slides through. The rotator cuff muscle becomes impinged especially when raising the arm horizontally or attempting to put a coat sleeve on. The good news is that after a detailed exam that includes range of motion of the neck, upper back, and shoulder followed by testing of all the muscles that cross the shoulder and palpating (clinically feeling) each structure a working diagnosis can be made and a treatment plan can be mapped out. If the “shoulder” problem is mechanical, and most of them are, a treatment plan that includes joint and muscle manipulation followed by therapeutic exercise at home, and health counseling can be made. The treatment plan will be a relationship between the practitioner and the patient and will consist of therapies in office and exercise prescription at home. Progress is the key! Great results can be expected within 4-6 weeks. Usually, treatments are 1-2 times a week and home therapies prescribed daily. Below are some pictures and treatments of the shoulder. This is a sample of some care and does not represent a treatment plan for the shoulder  Specific high velocity shoulder manipulation to the glenohumeral (shoulder) joint (this requires a high level of expertise and is only performed on certain conditions that warrant it- i.e. subluxation or impingement syndrome of shoulder)  Soft tissue manipulation to one of rotator cuff muscles (subscapularis) under the shoulder joint 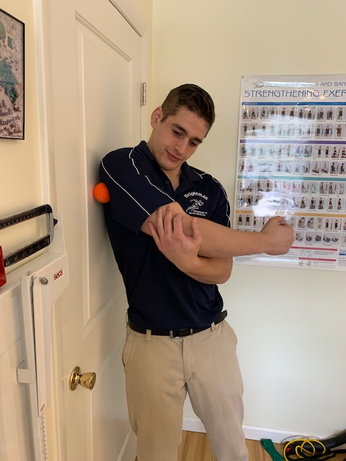 Myofascial release using a lacrosse ball (this can be part of self care at home- find the sore trigger points and gently apply pressure with the body over them for 5-10 seconds. Should feel slightly uncomfortable but a good pain. Pain scale when doing it should be a 3 or 4 out of 10. If it is a 5 out of 10 that is too much pressure. Therapeutic exercises for shoulder pain:
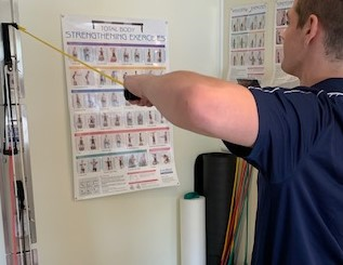
Assisted shoulder stretches(this is a general range of motion exercise)
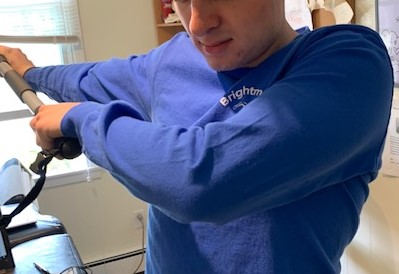
Rotator cuff theraband exercises (internal rotation)
Working both shoulders simultaneously develops symmetry
Dr. William Brightman DC, MS, MEd Chiropractor & Exercise Physiologist Private Practice in Mahopac
2 Comments
|
AuthorDr. William Brightman has been a practicing chiropractic physician since 1998 and has been in health promotions since 1989. He currently has a successful private practice in Mahopac, NY, where he specializes in the diagnosis and treatment of joint and muscle pain. ArchivesCategories
All
|










 RSS Feed
RSS Feed
